

660nm versus 850nm Infrared Light and their Benefits
 Wavelength: 660nm infrared light falls within the red portion of the electromagnetic spectrum, close to the visible light range. It is sometimes referred to as “red light therapy” and is visible as a deep red color. This wavelength is associated with stimulating cellular processes and promoting superficial tissue repair and rejuvenation.
Wavelength: 660nm infrared light falls within the red portion of the electromagnetic spectrum, close to the visible light range. It is sometimes referred to as “red light therapy” and is visible as a deep red color. This wavelength is associated with stimulating cellular processes and promoting superficial tissue repair and rejuvenation.
850nm infrared light is located in the near-infrared portion of the spectrum, just beyond the visible red range. It is invisible to the human eye and is often used for applications requiring deeper tissue penetration. This wavelength can reach structures deeper within the body, including muscles, joints, and organs.
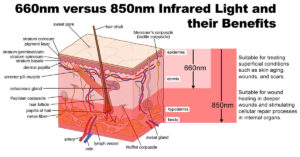
Penetration Depth: 660nm infrared light has a relatively shallow penetration depth compared to 850nm light. It can penetrate through the skin and reach tissues located within a few millimeters to a centimeter beneath the surface. This makes it suitable for treating superficial conditions such as skin aging, wounds, and scars.
850nm infrared light penetrates deeper into tissues, reaching depths of several centimeters or more depending on factors such as tissue composition and absorption properties. This makes it effective for addressing conditions that involve deeper structures, including muscles, tendons, joints, and even organs. Click here to order.
Biological Effects: 660nm infrared light stimulates cellular processes such as collagen synthesis and cellular metabolism [i], ATP production[ii]. It promotes wound healing and tissue repair[iii], which is skin rejuvenation by enhancing fibroblast by increasing blood flow, and reducing inflammation.
850nm infrared light affects deeper tissues and can penetrate through muscles, tendons, and joints. It promotes muscle recovery, pain relief, and inflammation reduction by improving circulation, increasing oxygenation, and modulating cellular signaling pathways involved in tissue repair and regeneration[iv]. Photobiomodulation (PBM) enhanced locomotion and muscle function. Following muscle injury, markers such as TBARS, protein carbonyls, superoxide dismutase, glutathione peroxidase, and catalase showed elevated levels, which were mitigated by PBM. PBM also prevented the elevation of IL-6 and IL-10 while reversing the trauma-induced decrease in brain-derived neurotrophic factor (BDNF) and vascular endothelial growth factor (VEGF)[v].
Therapeutic Applications[vi]: 660nm infrared light is commonly used for cosmetic and dermatological applications, including skin rejuvenation, wrinkle reduction, and scar treatment[vii]. It is also used for wound healing, acne treatment, and pain relief in superficial tissues.
850nm infrared light is utilized for deeper tissue applications, such as muscle recovery, sports injuries, joint pain, and inflammatory conditions. It is also used for promoting wound healing in deeper wounds and stimulating cellular repair processes in internal organs. Click here to order.
Clinical Considerations: When choosing between 660nm and 850nm infrared light for therapy, clinicians consider factors such as the depth of the target tissue, the desired biological effects, and the specific condition being treated.
In general, superficial conditions may benefit more from 660nm light, while deeper tissues and structures may require the deeper penetration provided by 850nm light.
Safety and Side Effects: Both 660nm and 850nm infrared light therapy are considered safe when used appropriately, with minimal risk of adverse effects. However, it’s essential to follow recommended guidelines for treatment duration, intensity, and distance to minimize the risk of overexposure or skin damage.
Side effects are rare but may include temporary redness, warmth, or mild discomfort at the treatment site. These typically resolve quickly and are not cause for concern.
In summary, 660nm and 850nm infrared light offer distinct advantages and can be used effectively for various therapeutic purposes. While 660nm light is suitable for superficial tissue applications and skin rejuvenation, 850nm light penetrates deeper into tissues and is beneficial for addressing conditions involving deeper structures. The choice between these wavelengths depends on factors such as the target tissue depth, desired biological effects, and specific therapeutic goals. Click here to order.
NEXT: 10Hz versus 40Hz Infrared Light. What is the differences and benefits?
Citations
[i] Zhang P, Zhang X, Zhu H. Photobiomodulation at 660 nm promotes collagen synthesis via downregulation of HIF-1α expression without photodamage in human scleral fibroblasts in vitro in a hypoxic environment. Graefes Arch Clin Exp Ophthalmol. 2023 Sep;261(9):2535-2545. doi: 10.1007/s00417-023-06066-5. Epub 2023 Apr 19. PMID: 37074407.
[ii] Quirk BJ, Sannagowdara K, Buchmann EV, Jensen ES, Gregg DC, Whelan HT. Effect of near-infrared light on in vitro cellular ATP production of osteoblasts and fibroblasts and on fracture healing with intramedullary fixation. J Clin Orthop Trauma. 2016 Oct-Dec;7(4):234-241. doi: 10.1016/j.jcot.2016.02.009. Epub 2016 Mar 10. PMID: 27857496; PMCID: PMC5106470.
[iii] https://www.researchgate.net/publication/282584922_Effect_of_660_nm_Light-Emitting_Diode_on_the_Wound_Healing_in_Fibroblast-Like_Cell_Lines
[iv] Hamblin MR. Mechanisms and applications of the anti-inflammatory effects of photobiomodulation. AIMS Biophys. 2017;4(3):337-361. doi: 10.3934/biophy.2017.3.337. Epub 2017 May 19. PMID: 28748217; PMCID: PMC5523874.
[v] Hamblin MR, et al
[vi] Wunsch A, Matuschka K. A controlled trial to determine the efficacy of red and near-infrared light treatment in patient satisfaction, reduction of fine lines, wrinkles, skin roughness, and intradermal collagen density increase. Photomed Laser Surg. 2014 Feb;32(2):93-100. doi: 10.1089/pho.2013.3616. Epub 2013 Nov 28. PMID: 24286286; PMCID: PMC3926176.[vii] Wunsch A, et al